 Acne.org Products
Acne.org Products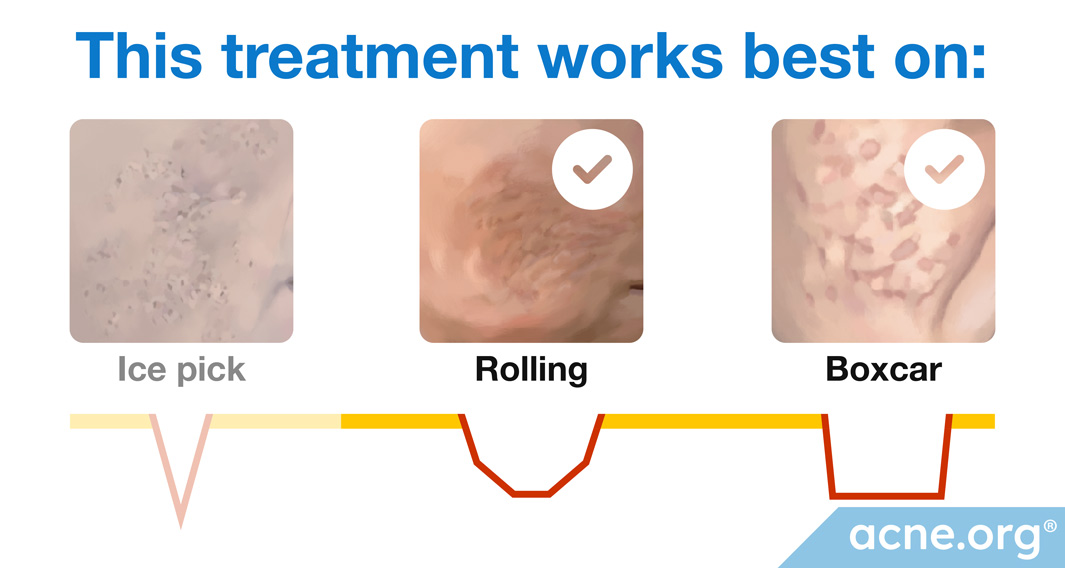
* Laser resurfacing works best for boxcar and rolling scars.
Laser resurfacing is a non-invasive procedure (does not involve cutting or inserting tools into the skin) that consists of shining an intense beam of light onto the skin. Because the light is concentrated and intense, it causes controlled damage to the skin. The type and extent of the skin damage depends on the type of laser. This controlled damage aims to stimulate skin healing and/or regrowth, which results in a smoother and more even skin surface–in other words, the skin is “resurfaced.”
Lasers can be non-ablative or ablative. Non-ablative lasers create a controlled injury deep in the skin, whereas ablative lasers completely ablate (remove) the surface of the skin.
Lasers can also be non-fractional or fractional. Non-fractional lasers, also known as non-fractionated lasers, treat the whole skin surface in a particular area without leaving any gaps. Because an entire section of skin is damaged, healing time is longer than with fractional lasers. Fractional lasers deliver many small pinpoints of laser light in a grid-like pattern so that areas of skin in-between the pinpoints are left untouched. 1
Non-ablative (non-skin-removing) non-fractional lasers: These lasers work by causing a controlled injury in the dermis (the deep layer of the skin), which triggers skin remodeling and the formation of new collagen in the dermis. Because non-ablative non-fractional lasers cause the skin to slowly reshape itself from the inside, the results they achieve are more gradual and moderate compared to ablative non-fractional lasers, but they offer the advantages of a short recovery time and a relatively low risk of side effects.2
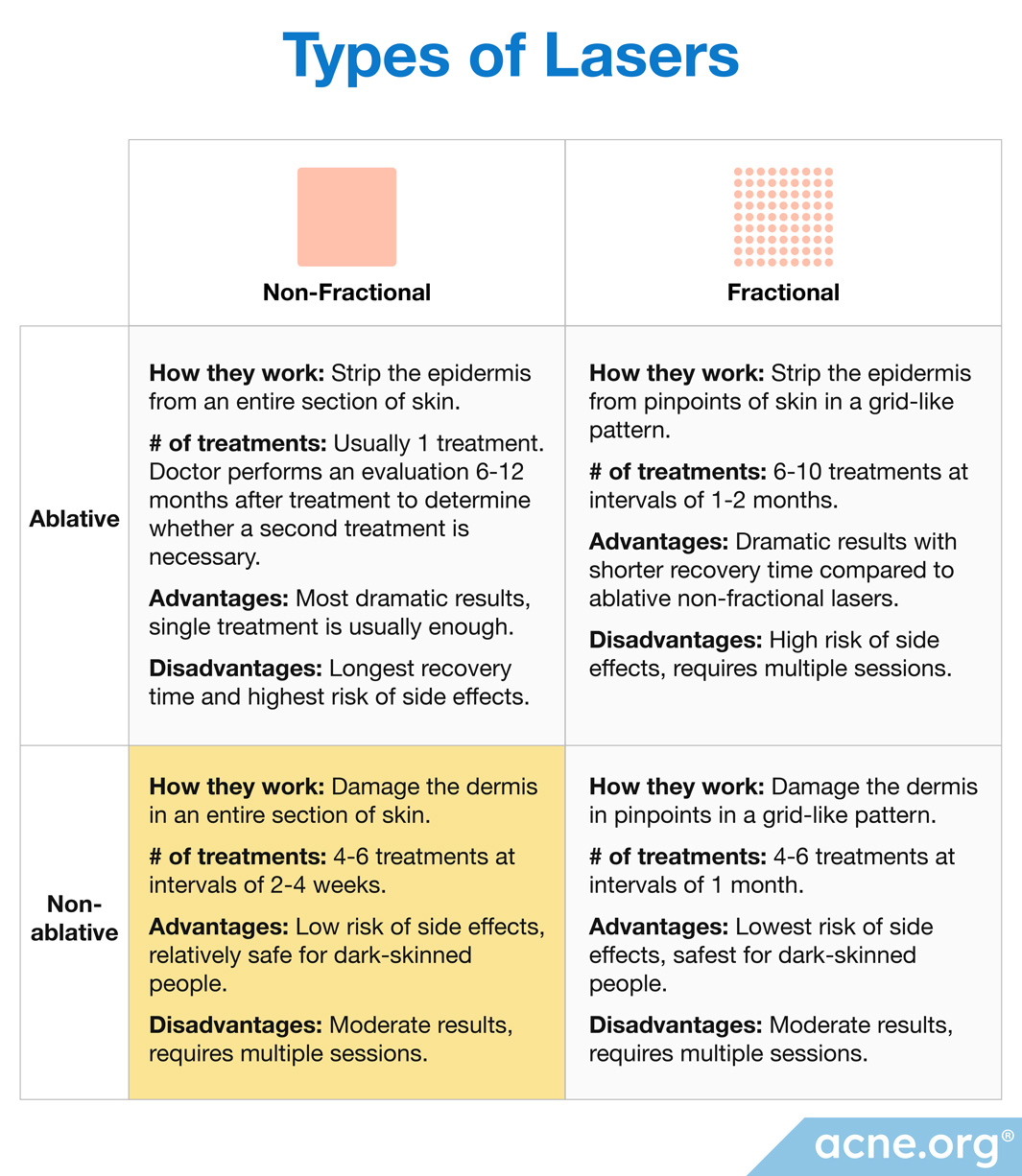
Non-ablative Non-fractional lasers:
- How they work: Damage the dermis in an entire section of skin
- # of treatments: 4-6 treatments at intervals of 2-4 weeks
- Advantages: Low risk of side effects, relatively safe for dark-skinned people2
- Disadvantages: Moderate results, requires multiple sessions2
There are many different subtypes of lasers, each named after the material it is made with. Lasers can be created using glass, crystals, or gasses, and the specific material determines the color of the laser light.2
The materials in lasers used for non-ablative non-fractional skin resurfacing include:
- Er:glass (erbium glass) laser
- Nd:YAG (neodymium:yttrium-aluminum-garnet) laser
- Diode laser
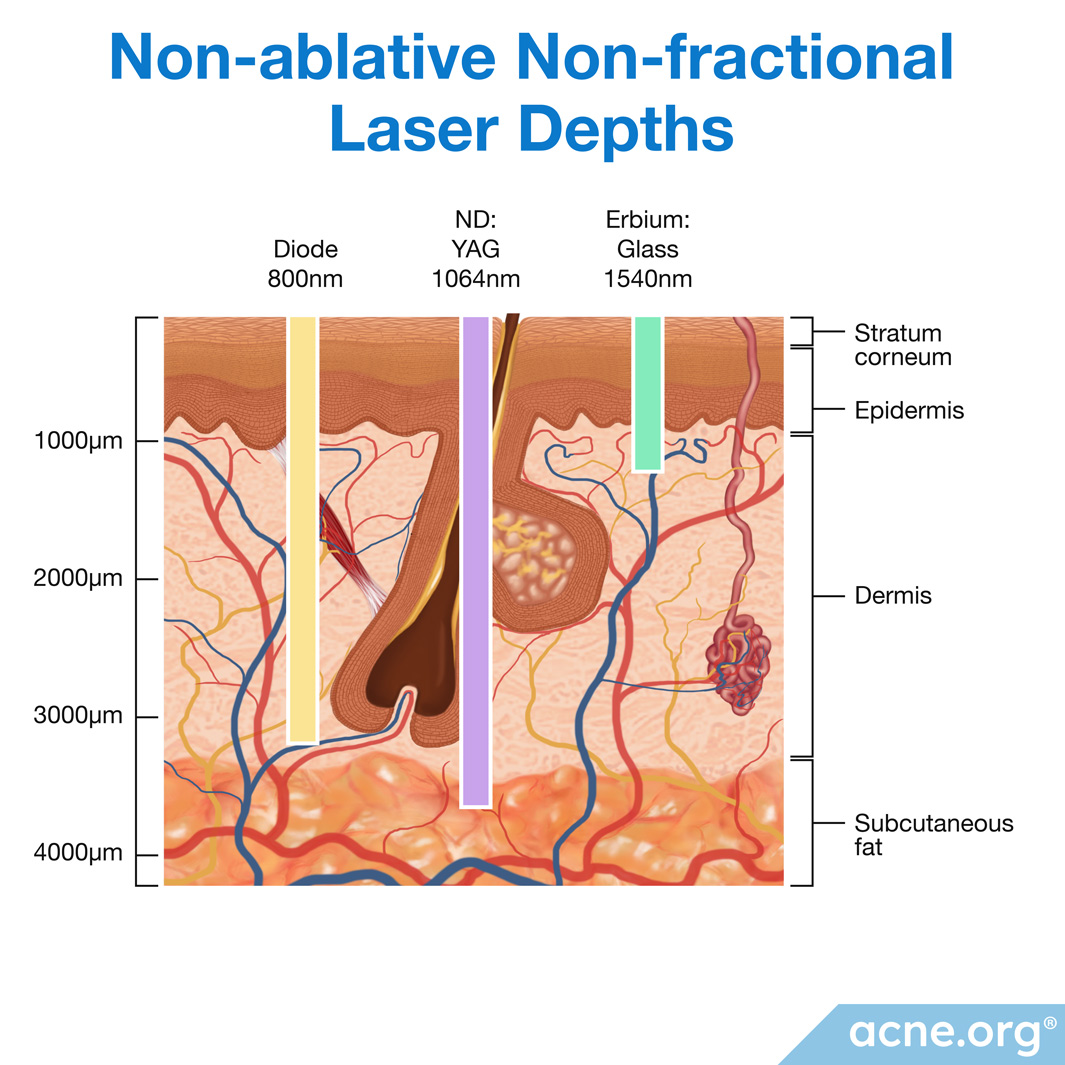
Each laser subtype penetrates the skin to a different depth. In general, ablative lasers do not penetrate deep into the dermis:1
- Er:glass non-fractional laser: Does not go as deep into the dermis as diode and Nd:YAG (neodymium:yttrium-aluminum-garnet) laser
- Diode non-fractional laser: Does not go as deep into the dermis as Nd:YAG (neodymium:yttrium-aluminum-garnet) laser
- Nd:YAG (neodymium:yttrium-aluminum-garnet) non-fractional laser: Goes deeper into the dermis than the diode laser, all the way downt to the subcutaneous fat layer
As with all scar revision treatments, laser resurfacing is sometimes combined with other scar revision procedures to attain desired results.
People with active acne should not undergo acne scar repair of any kind, including laser resurfacing. Make sure your skin is completely clear of acne before beginning scar treatment.
Laser resurfacing cannot be performed while there is an active skin infection or skin condition such as a bacterial infection, eczema, or psoriasis. Ensure your skin is clear before seeking laser resurfacing.1
Doctors do not recommend undergoing laser scar treatment for 6 months after taking oral isotretinoin (Accutane®), because during this time, the skin may respond unpredictably to laser treatment.1
If you have a history of keloid scarring, approach laser resurfacing with caution, as you may have a higher chance of developing keloid scars as a side effect of laser resurfacing.1
Patients with darker skin are at increased risk of pigmentation (skin coloring) due to laser treatment, especially hyperpigmentation (skin darkening).
Before agreeing to undergo laser resurfacing, discuss your treatment options, expected outcomes, and treatment prices with multiple doctors.
Procedure details:

Before booking your treatment, your doctor should first schedule a session to discuss the procedure, expected results, and possible complications with you and to answer your questions.
If you are planning to undergo treatment with an ablative laser, your doctor may prescribe antiviral medications for you to take before the procedure in order to prevent a viral skin infection from developing after treatment.
Laser resurfacing is usually performed in an outpatient setting. During the treatment, the doctor will give you protective eyewear to prevent the laser from damaging your eyes.
No matter which type of laser your doctor uses, she will have to fine-tune the laser settings in order to get the best results while minimizing recovery time and side effects. Once the settings are dialed in, she will make several passes over your scar with the laser, which produces mild pain.
In general, ablative lasers cause more skin damage than non-ablative lasers. Still, how much skin damage any given laser produces can vary significantly depending on several variables.
One of these variables is the wavelength that the laser material creates:
- Wavelength: Each type of material creates a laser with a specific wavelength. The wavelength of a laser is a number in nm (nanometers) corresponding to a specific color of light. Most lasers used for skin resurfacing emit colors of light that are invisible to the human eye, so you will not be able to see the laser beam during your treatment. For example, a diode laser emits infrared light with a wavelength of about 800 nm, which you cannot see, but may feel as heat during treatment.
| Wavelength | |
| Non-ablative lasers | Nd:YAG – 1,064 nm Diode – 810 nm Er:glass – 1,540 nm |
Other settings that determine how much damage a laser causes can be controlled by the doctor:
- Delivered fluence, also known as energy density: Fluence or energy density is a measure of how much energy the laser delivers per unit area of the skin–in other words, how intense the laser is. It is important for the doctor to set the fluence high enough to cause a controlled injury to the skin, but not so high as to create unnecessary damage. The doctor may need to set the fluence higher to target a particularly strong or large structure, like a severe or wide scar. Delivered fluence only depends on the doctor’s settings, not on the type of laser.
- Pulse duration: Normally, the light from a laser is delivered in a series of short bursts, called pulses, with short breaks in-between. Pulse duration is a measure of how long each pulse lasts. The longer the pulse, the more skin damage it causes, so this is another setting that the doctor needs to carefully fine-tune in order to obtain the best results and minimize the side effects. Just like delivered fluence, pulse duration only depends on the doctor’s settings, not on the type of laser.
Anesthesia:
Laser scar treatment can be uncomfortable and even painful. To numb your skin before the procedure, your doctor may:
- Inject a local anesthetic into your skin before beginning treatment
- Apply a topical anesthetic to your skin 30-60 minutes before the treatment
- Provide you with a topical anesthetic to apply to your skin before you arrive at the doctor’s office for your treatment3-7
Before-and-after:

Acne scars before (left) and after 4 treatments (right) with non-ablative non-fractional laser.
References
- Sobanko JF, and Alster TS. Management of acne scarring, part I: a comparative review of laser surgical approaches. Am J Clin Dermatol. 13(5), 319-30 (2012)
- Preissig J, Hamilton K, and Markus R. Current laser resurfacing technologies: A review that delves beneath the surface. Semin Plast Surg. 26(3), 109–116 (2012).
- Alexis AF, et al. Nonablative Fractional Laser Resurfacing for Acne Scarring in Patients With Fitzpatrick Skin Phototypes IV-VI. Dermatol Surg. 42(3), 392-402 (2016).
- Alster TS, and West TB. Resurfacing of atrophic facial acne scars with a high-energy, pulsed carbon dioxide laser. Dermatol Surg. 22(2), 151-4 (1996).
- Bhatia AC, Dover JS, Arndt KA, Stewart B, and Alam M. Patient satisfaction and reported long-term therapeutic efficacy associated with 1,320 nm Nd:YAG laser treatment of acne scarring and photoaging. Dermatol Surg. 32(3), 346-52 (2006).
- Chae WS, et al. Comparative study on efficacy and safety of 1550 nm Er:Glass fractional laser and fractional radiofrequency microneedle device for facial atrophic acne scar. J Cosmet Dermatol. 14(2), 100-6 (2015).
- Chae WS, et al. Comparative study on efficacy and safety of 1550 nm Er:Glass fractional laser and fractional radiofrequency microneedle device for facial atrophic acne scar. J Cosmet Dermatol. 14(2), 100-6 (2015).
Future reading
- Ahmed R, Mohammed G, Ismail N, and Elakhras A. Randomized clinical trial of CO₂ LASER pinpoint irradiation technique versus chemical reconstruction of skin scars (CROSS) in treating ice pick acne scars. J Cosmet Laser Ther. 16(1), 8-13 (2014).
- Engın B, et al. Evaluation of effectiveness of erbium:yttrium-aluminum-garnet laser on atrophic facial acne scars with 22-MHz digital ultrasonography in a Turkish population. J Dermatol. 39(12), 982-8 (2012).
- Jeong JT, and Kye YC. Resurfacing of pitted facial acne scars with a long-pulsed Er:YAG laser. Dermatol Surg. 27(2), 107-10 (2001).
- Lee SJ, Kang JM, Chung WS, Kim YK, and Kim HS. Ablative non-fractional lasers for atrophic facial acne scars: a new modality of erbium:YAG laser resurfacing in Asians. Lasers Med Sci. 29(2), 615-9 (2014).
- Wanitphakdeedecha R, Manuskiatti W, Siriphukpong S, and Chen TM. Treatment of punched-out atrophic and rolling acne scars in skin phototypes III, IV, and V with variable square pulse erbium:yttrium-aluminum-garnet laser resurfacing. Dermatol Surg. 35(9), 1376-83 (2009).
- Tanzi EL, and Alster TS. Treatment of atrophic facial acne scars with a dual-mode Er:YAG laser. Dermatol Surg. 28(7), 551-5 (2002).
- Bjørn M, Stausbøl-Grøn B, Braae Olesen A, and Hedelund L. Treatment of acne scars with fractional CO2 laser at 1-month versus 3-month intervals: an intra-individual randomized controlled trial. Lasers Surg Med. 46(2), 89-93 (2014).
- Cho SB, Lee SJ, Kang JM, Kim YK, Chung WS, and Oh SH. The efficacy and safety of 10,600-nm carbon dioxide fractional laser for acne scars in Asian patients. Dermatol Surg. 35(12),1955-61 (2009).
- Hedelund L, Haak CS, Togsverd-Bo K, Bogh MK, Bjerring P, and Haedersdal M. Fractional CO2 laser resurfacing for atrophic acne scars: a randomized controlled trial with blinded response evaluation. Lasers Surg Med. 44(6), 447-52 (2012).
- Majid I, and Imran S. Fractional CO2 Laser Resurfacing as Monotherapy in the Treatment of Atrophic Facial Acne Scars. J Cutan Aesthet Surg. 7(2), 87-92 (2014).
- Manuskiatti W, Triwongwaranat D, Varothai S, Eimpunth S, and Wanitphakdeedecha R. Efficacy and safety of a carbon-dioxide ablative fractional resurfacing device for treatment of atrophic acne scars in Asians. J Am Acad Dermatol. 63(2), 274-83 (2010).
- Manuskiatti W, Iamphonrat T, Wanitphakdeedecha R, Eimpunth S. Comparison of fractional erbium-doped yttrium aluminum garnet and carbon dioxide lasers in resurfacing of atrophic acne scars in Asians. Dermatol Surg. 39(1 Pt 1), 111-20 (2013).
- Nirmal B, et al. Efficacy and safety of erbium-doped yttrium aluminium garnet fractional resurfacing laser for treatment of facial acne scars. Indian J Dermatol Venereol Leprol. 79(2), 193-8 (2013).
- Wang YS, Tay YK, and Kwok C. Fractional ablative carbon dioxide laser in the treatment of atrophic acne scarring in Asian patients: a pilot study. J Cosmet Laser Ther. 12(2), 61-4. (2010).
- Yuan XH, Zhong SX, and Li SS. Comparison study of fractional carbon dioxide laser resurfacing using different fluences and densities for acne scars in Asians: a randomized split-face trial. Dermatol Surg. 40(5), 545-52 (2014).
- Zhang Z, Fei Y, Chen X, Lu W, and Chen J. Comparison of a fractional microplasma radio frequency technology and carbon dioxide fractional laser for the treatment of atrophic acne scars: a randomized split-face clinical study. Dermatol Surg. 39(4), 559-66 (2013)
- Cachafeiro T, Escobar G, Maldonado G, Cestari T, and Corleta O. Comparison of Nonablative Fractional Erbium Laser 1,340 nm and Microneedling for the Treatment of Atrophic Acne Scars: A Randomized Clinical Trial. Dermatol Surg. 42(2), 232-41 (2016).
- Isarría MJ1, Cornejo P, Muñoz E, Royo de la Torre J, and Moraga JM. Evaluation of clinical improvement in acne scars and active acne in patients treated with the 1540-nm non-ablative fractional laser. J Drugs Dermatol.10(8), 907-12 (2011).