 Acne.org Products
Acne.org Products3 hours ago, guitarman01 said:These are pretty direct connections. The rest I will get into later when I have more time.Impact of 6-month course of 1 mg finasteride tablets on levels of lipid profile in men with androgenic alopecia
http://www.endocrine-abstracts.org/ea/0029/ea0029p277.htmAtherosclerosis constitutes one of the most frequent diseases and one of the important predisposing factor for atherosclerosis is lipid profile change.
Findings: A significant decreases in fasting plasma level of HDL was observed after 6 months of therapy (P<0.001). Moreover, a statistically significant rise in fasting plasma level of triglyceride was observed after 3 months of therapy
Conclusion: Our study demonstrated for the first time that using 1mg finasteride tablets to treat androgenic hair loss may lead to complications of the lipid profile through reducing HDL and increasing total cholesterol. Finasteride may decrease dihydrotestosterone and increased testosterone this change in lipid profile may be due to testosterone elevation by using finasteride.
"Thatisotretinoincan cause worsening of lipids with significant increases in total cholesterol and triglycerides is well known," he commented; however, "the mechanism of retinoid-associateddyslipidemiahas not been completely elucidated."Aug 22, 2006You can look at various examples of vascular disease and nervous system deterioration going hand in hand.
Again this is coming directly from the Accutane pamphlet.
"May cause blood vessel inflammation."
We know what people have looked into extensively already, I have an idea what they haven't.
All of this isnt guaranteed to stay true over a period of time, but it might start to paint a picture.
I appreciate that. Its no surprise that powerful drugs like accutane or propecia have effects on things like your lipid profile or cause inflammation. Firstly, the most important question here is are these kinds of peripheral effects present a year or two after stopping the treatments. Its possible but I doubt it.
Secondly, even if they are present I still struggle to see how things like changes in lipid levels or even blood vessel inflammation could account for the severe, persistent effects of post accutane syndrome (PAS) such as depression, sexual dysfunction, anhedonia and depersonalisation to name just a few. I don't say its impossible, I just find it highly improbable and fail to think of any obvious links between the side effects and condition. As opposed to the other potential causes of PAS which hold far more weight.
Thirdly, when listing the effects of accutane. Its very important to distinguish between effects which occur whilst on the drug and those which persist beyond treatment as these are very different things. And a lot of time and energy is wasted focusing on the wrong aspect of this condition/syndrome. Not to mention money which would be better spent supporting a project like the RxISK prize - https://rxisk.org/prize/
A useful exercise to undertake when analysing the side effects of Accutane or Propecia or SSRI's is to look for other drugs which also cause similar side effects. I'll bet I could find you a 100 other drugs which alter lipid levels and cause blood vessel inflammation, perhaps to a greater degree than Accutane which don't cause the persisting symptoms of PAS. Through this kind of process of elimination we can start to identify what is more or less likely to be the cause.
Also I don't want this to come across as if I'm trying to prove you wrong or argue here. I respect and appreciate anyone who is researching these issues and PAS. We are all in this together and will only find a cure if we are organised and work with each other.
On 2/27/2018 at 1:47 AM, TrueJustice said:Has anyone thought to just supplement testosterone?
I was about to a few years ago when seeing 2 different doctors but went down the gastro path instead......and here I still am
Compound pharmacies can make it up I believe. If that doesnt do anything Im not sure what will....
I have experimented with testosteone ethanate, I used between 300mg/week up to 600mg/week over an 8-10 week period. I had large increases in muscle mass, strength and recovery. But almost zero changes in mood or libido. To me, this indicates either a a dysfunction with the androgen receptor, the dopamine system itself or a problem with the serotonin signalling suppressing dopamine as in PSSD.
So something caught my eye that may have gone unnoticed from my very first blood draw (didnt include the hormones I just recently got)
My monocytes were 11% (no reference range on my sheet was displayed)
and absolute were 0.7 with a reference range of 0.3-0.9 ...
Dont these seem slightly elevated?
And doesnt low t cause elevated monocytes?
Glucose, Serum 93 mg/dL 65 - 99
DYSAUTONOMIA EVALUATION SERUMPositive
Tested positive for acetylcholine ganglionic neuronal antibody
HDL Cholesterol 43 mg/dLReference is greater than >39 This is very low(major cardiovascular risk factor) the higher the better, should be in the 60s
CARDIAC STRESS TEST
Abnormal ECG response to stress. 2 mm flat depressed ST segment in leads
III occuring in Stage 2 using Bruce protocol. The patient exercised for
11 mins. Persisting up to 3 minutes into recovery.
EKG 12-LEAD
POSSIBLE LEFT ATRIAL ENLARGEMENT
Dilute Russell Viper Venom Screen
ABNORMAL
MRI BRAIN WO IV CONTRAST
There is mild
volume loss of brain parenchyma, advanced for patient's age.
There is thinning of the body of the corpus
callosum. This finding is stable compared to prior MRI, 8/10/2013.
@flynn
This is what im talking about when looking at painting a picture.
@mariovitali
I know you have alot of 23andme data
Have you looked at these genes?
Apolipoprotein EApoEstatus is technically defined by two different SNPs,rs429358andrs7412.
rs7412
rs429358
Apolipoprotein E (ApoE) is a class of proteins involved in the metabolism of fats in the body. It is important in Alzheimer's disease and cardiovascular disease. Lipoproteins are molecules composed of fats and proteins.
rs429358 is the main gene tested for the e4 variant from 23andme
IM 3/4 APOE Genotype. Anyone else?
Lipid biosynthesis (shown to be dysregulatedduring Accutane and Propecia treatment)
Protein involved in the synthesis of lipids, a diverse class of compounds which are insoluble in water but soluble in organic solvents. They include fats, oils, triacylglycerols, fatty acids, glycolipids, phospholipids and steroids.
Warfarin dose related to apolipoprotein E (APOE) genotype.
https://www.ncbi.nlm.nih.gov/pubmed/15952022
Previous studies have shown that individuals carrying the APOE*E4 allele have a faster uptake of lipoproteins into the liver and lower levels of circulating vitamin K than others.
This is a copy/paste from my Cohort for these two Genes :
{'snp': 'rs7412', 'homozygous': 0.0, 'heterozygous': 12.07, 'not_in_chip': 0.0, 'no_mutation': 87.93}{'snp': 'rs429358', 'homozygous': 3.45, 'heterozygous': 24.14, 'not_in_chip': 3.45, 'no_mutation': 68.97}APOE has been mentioned here :
12 hours ago, flynn said:I have experimented with testosteone ethanate, I used between 300mg/week up to 600mg/week over an 8-10 week period. I had large increases in muscle mass, strength and recovery. But almost zero changes in mood or libido. To me, this indicates either a a dysfunction with the androgen receptor, the dopamine system itself or a problem with the serotonin signalling suppressing dopamine as in PSSD.
This doesn't mean you should write off hormones, even if it forms only part of your recovery.
The following is all assuming youve had levels tested and results were low, for your age.
First, 300-600mg Test E is a very high dose.
For medical purposes (ie TRT) , standard doses are 100-200mg/per week.
There are many TRT guys and even more on bodybuilding doses who seem to notice libido tanks, despite muscle gains, and these guys didn't take accutane either. That's why bodybuilders , for e.g. also run auxillaries such as aromatase inhibitors and dopamine agonists.
The first step would be to reduce doses to appropriate TRT levels and then closely monitor any parameters which may be causing low libido (ie Estradiol levels).
5 hours ago, mikez said:This doesn't mean you should write off hormones, even if it forms only part of your recovery.The following is all assuming youve had levels tested and results were low, for your age.
First, 300-600mg Test E is a very high dose.
For medical purposes (ie TRT) , standard doses are 100-200mg/per week.
There are many TRT guys and even more on bodybuilding doses who seem to notice libido tanks, despite muscle gains, and these guys didn't take accutane either. That's why bodybuilders , for e.g. also run auxillaries such as aromatase inhibitors and dopamine agonists.
The first step would be to reduce doses to appropriate TRT levels and then closely monitor any parameters which may be causing low libido (ie Estradiol levels).
I agree bro. We can't cancel out any options. But I'm fairly certain testosterone levels aren't the problem. 300mg/week is high but its not ridiculously high. Surely I would have felt some change in sex drive/libido. From what I remember I barely noticed any mental changes which seems highly unusual to me. Even if my libido wasn't altered, people usually feel mentally different i.e. more alpha from taking steroids. I agree that knowing estrogen would have been useful, its one test that I still need to get. But I'm pretty sure I've seen people with PAS report normal estrogen levels.
There are also quite a few other guys with PAS who have tried steroids but reported no improvement. I imagine that by this stage, if steroids/TRT helped, someone or more people would have reported it as helping their sexual dysfunction.
These effects seem too ingrained and long term to be simply down to androgen levels. Though I do still think, a down regulation of androgen receptors is a possibility.
Note from my tests, that my testosterone is very healthy. Only abnormal result is DHEA-S which is very high but again this should lead to higher sex drive/libido not lower. I've also had thyroid checked (all normal). The expensive tests I've had to save other people wasting money are Growth hormone, IGF-1 and IGFBP-3
Here are some recent blood tests, these are my normal levels (not on supplements/steroids etc.):
D.H.E.A. Sulphate* 16.8 umol/L 0.44 - 13.4
FOLLICLE STIM. HORMONE 3.0 IU/L 1.5 - 12.4
LUTEINISING HORMONE 5.2 IU/L 1.7 - 8.6
TESTOSTERONE 25.1 nmol/L 7.6 - 31.4
Reference Ranges apply to adults
SEX HORMONE BINDING GLOB 46 nmol/L 16 - 55
Testosterone/SHBG Ratio 54.6 24 104
THYROID STIMULATING HORMONE 1.48 mIU/L 0.27 - 4.2
FREE THYROXINE 16.0 pmol/l 12.0 - 22.0
FREE T3 5.6 pmol/L 3.1 - 6.8
https://www.gov.uk/drug-safety-update/isotretinoin-risk-of-serious-skin-reactions
Does anyone know if this is listed in the PIL.
If anyone is taking accutane at the moment can you check.
I am also interested to know if the sexual side are being listed yet.
My own research suggests not but I have been told by the regulators that it is.
About 10 percent of people withStevens-Johnson syndromedie from thedisease, while the condition is fatal in up to 50 percent of those with toxic epidermal necrolysis.
12 hours ago, mariovitali said:This is a copy/paste from my Cohort for these two Genes :
{'snp': 'rs7412', 'homozygous': 0.0, 'heterozygous': 12.07, 'not_in_chip': 0.0, 'no_mutation': 87.93}{'snp': 'rs429358', 'homozygous': 3.45, 'heterozygous': 24.14, 'not_in_chip': 3.45, 'no_mutation': 68.97}
Is this free software? Id like to see how this is being looked at.
I have another snp to look at. It has to do with Vitamin K cycling.
rs9934438
Vitamin K epoxide reductase complex subunit 1 (VKORC1) polymorphism and aortic calcification: the Rotterdam Study.
https://www.ncbi.nlm.nih.gov/pubmed/18218987?dopt=Abstract
Persons with at least one T-allele had a statistically significant 19% (95% CI 2 to 40%) risk increase of calcification
The T-allele of the VKORC1 1173C>T polymorphism was associated with a significantly higher risk of aortic calcification in Whites.
How about yourself on these?
Im TT (or AA)
Persons with a T-allele have a lifelong reduced activity of VKORC1.
Effects from this are expected in extrahepatic proteins such as MGP because -carboxylation here fully depends on VKORC
On 3/7/2018 at 8:03 AM, flynn said:Yes but its possible that if people metabolise vit A in a significantly different way due to some gene variant etc. Than during accutane treatment they would be exposed to far higher dosages than other people, and the risks associated with vit A ability to alter gene expression etc. would be greatly enhanced. Which would explain why only a subset of patients develop PAS. Alternatively people with PAS may just have a set of genes which make them far more susceptible to developing PAS. We will never know the answer to this question until genome sequencing becomes cheap enough, so that all PAS people can get their genes sequenced.Well if PFS and PAS share a common underlying cause such as 5AR inhibition. It doesn't seem like accutane has as much of a direct effect on 5AR, and its action on 5AR (if it has any) is relatively small. However if metabolism in PAS sufferers is different and they get a huge dose of accutane metabolites, this may make accutanes effect on 5AR substantial enough to cause PAS.
Whole-genome sequencing is, or will soon be, cheap enough. The greater problem will be to find someone to officially analyze the data in the context of a scientific study; that is if there are enough volunteers getting tested among the post-Accutane community to generate a sufficient amount of data to be considered significant. And of course, there will be pompous dermatologists scoffing at the study anyway since it would be patient-generated data. Not as if their opinions would matter if we got a clean-cut set of genes that indicated an increased risk of side effects and possible therapeutic targets.
Also, Accutane has little effect on circulating DHT levels, BUT a profound effect on peripheral 5ar activity. This is true of studies of skin biopsies taken after treatment and one study of type-1 5ar in the prostate during treatment.
There's reason to believe the negative effects of Accutane on 5ar-I observed in skin biopsies extend to the brain and central nervous system as seen in PFS. It's a shame that animal studies have not been performed on this point yet, but I would feel bad for any animal who was turned into a creature like me.
.... Noticed your DHEA-S was over the top high. That seems to be an almost across-the-board trait of post-Accutane people. Not sure why. ...Maybe persistently reduced negative feedback in HPA-axis as seen in the Accutane+Mifepristone study posted a few weeks ago?
8 hours ago, hatetane said:Actually I just found this, So I am assuming all PILS must now been up-to-date.
Asour health minster kindly quoted
"Let us be frank: there is risk in taking an aspirin or a paracetamol, and more sophisticated drugs carry even more risks.
Have you also confirmed the risk of sexual and reproductive side-effects are finally being printed on the PILS of all newly-manufactured boxes of Isotretinoin sold in Europe?
Seems pharmaceutical companies don't like to change the labels until they are coerced into doing it. Especially Roche.
anyone ever bother asking these guys if their sides of low t went away after TRT...?
I did TRT last year from March to December. My blood tests showed low FSH and low T, which is a common pattern from what I've gathered from "taned brains" over the years. I'm fortunate enough to not have full on ED, but my libido was definitely a shadow of what it was pre tane. Yea, TRT is great...it makes your muscles feel tighter, your whole body tighter, leaner...erections upon waking up and a couple more throughout the day randomly. It's not bad being in the 1000 range when you've been at 200 for the past several years. My levels were so high towards the end of the cycle that the blood test couldn't even read the level, it just said >1000. It's pretty cool. But, it doesn't absolve clinical depression fully (at least for me). Although, cannabis has been helping lately, and I can tolerate more and more of it each day that goes by, which tells me I'm making improvements with my neurology.
When I asked my endo if there was a way to bring up FSH, he said no, there was not. however...
HMG is a fertility drug similar to HCG in use and some of its function, but also has the added benefit of FSH stimulation, while HCG is known mainly for LH stimulation. Your sex drive and sense of well being are restored as well as your potential for staying or becoming fertile (increased sperm count for men). The most significant difference between HCG and HMG is in the fact that HCG mimics LH (luetinized hormone). It gives the body a false signal that LH is present and everything else responds accordingly. HMG actually elevates natural LH. Now to some, theres little difference, but its always better when the body reacts in the most natural manner.
Well, regarding hormones, if that really is your priority, there is so much out there to try if you truly have a nothing to lose mentality. HCG, HMG, Test, HGH, Follistatin, Mifepristone, Clomid, oxytocin. And it is complicated. There's no right solution. The neuro endocrine system is super complex, so you either have to find an innovative knowledgeable physician that is willing to help (very difficult 1%) or you will have to trial and error on your own with the help of the internet (which isn't all bad if you find the right people/websites). I will try a couple of those on the list this spring/summer and try and give you my feedback, but I personally think my problems are more serotonin or dopamine related. But this summer should be fun. We will see.
8 hours ago, guitarman01 said:Is this free software? Id like to see how this is being looked at.I have another snp to look at. It has to do with Vitamin K cycling.
rs9934438Vitamin K epoxide reductase complex subunit 1 (VKORC1) polymorphism and aortic calcification: the Rotterdam Study.
https://www.ncbi.nlm.nih.gov/pubmed/18218987?dopt=Abstract
Persons with at least one T-allele had a statistically significant 19% (95% CI 2 to 40%) risk increase of calcification
The T-allele of the VKORC1 1173C>T polymorphism was associated with a significantly higher risk of aortic calcification in Whites.How about yourself on these?
Im TT (or AA)Persons with a T-allele have a lifelong reduced activity of VKORC1.
Effects from this are expected in extrahepatic proteins such as MGP because -carboxylation here fully depends on VKORC
I am homozygous. The software i use , i created it using Python and what it does is that it summarizes SNPs found in many 23andme DNA files.
Here are the results (all numbers are percentages) :
{'snp': 'rs9934438', 'homozygous': 18.97, 'heterozygous': 46.55, 'not_in_chip': 0.0, 'no_mutation': 34.48}Given that the MAF of this SNP is 35.58% we wish to know if these results are statistically significant. I will get back to you for this.An example of a "good catch" regarding Vitamin K are the following based on their statistical significance :MERTK rs13027171VKORC1 rs2884737 VKORC1 rs17708472
23 minutes ago, macleod said:I did TRT last year from March to December. My blood tests showed low FSH and low T, which is a common pattern from what I've gathered from "taned brains" over the years. I'm fortunate enough to not have full on ED, but my libido was definitely a shadow of what it was pre tane. Yea, TRT is great...it makes your muscles feel tighter, your whole body tighter, leaner...erections upon waking up and a couple more throughout the day randomly. It's not bad being in the 1000 range when you've been at 200 for the past several years. I was so high towards the end of my cycle that the blood test couldn't even read the level, it just said >1000. It's pretty cool. But, it doesn't absolve clinical depression fully (at least for me). Although, cannabis has been helping lately, and I can tolerate more and more of it each day that goes by, which tells me I'm making improvements with my neurology.
When I asked my endo if there was a way to bring up FSH, he said no, there was not. however...
HMG is a fertility drug similar to HCG in use and some of its function, but also has the added benefit of FSH stimulation, while HCG is known mainly for LH stimulation. Your sex drive and sense of well being are restored as well as your potential for staying or becoming fertile (increased sperm count for men). The most significant difference between HCG and HMG is in the fact that HCG mimics LH (luetinized hormone). It gives the body a false signal that LH is present and everything else responds accordingly. HMG actually elevates natural LH. Now to some, theres little difference, but its always better when the body reacts in the most natural manner.
Well, regarding hormones, if that really is your priority, there is so much out there to try if you truly have a nothing to lose mentality. HCG, HMG, Test, HGH, Follistatin, Mifepristone, Clomid, oxytocin. And it is complicated. There's no right solution. The neuro endocrine system is super complex, so you either have to find an innovative knowledgeable physician that is willing to help (very difficult 1%) or you will have to trial and error on your own with the help of the internet (which isn't all bad if you find the right people/websites). I will try a couple of those on the list this spring/summer and try and give you my feedback, but I personally think my problems are more serotonin or dopamine related. But this summer should be fun. We will see.
Hows the Lions Mane going??
I dont pretend to know as much as many of you here that post a lot of science and results etc but one area that we dont tend to dwell on enough is the nervous system and how it might be altered after tane. Sure weve discussed Vit B but what else can we look at??
I was listening to the radio today about people whove been bitten by venomous snakes who yes have lived to tell the tale ( no pun ) but are left with lingering nervous system issues years after, even little things like no sense of smell etc. My guess is you could substitute snake venom with Accutane - both are poisons yeah, both impact on the nervous system, Im suggesting we could have a problem with this system and we need to look into it more....
Macleod - you raised a similar point recently about the nervous system did you not, affected after tane?
Yes, I do Lion's Mane with my coffee. The brand is Real Mushrooms (suggested by Walden). I also take 1000mg of "Lypo-Spheric" Vit C. Both on amazon and the highest rated. You really can't go wrong with Vitamin C as a daily supplement. Also, I am taking Arginine in supplement form as it is still cold weather where I live and I need better circulation to my fingertips. Perhaps it is helping create better circulation in the brain, who knows. Last month I was taking both B1 and B12, but I've run out. I still take Vitamin D occasionally. There's really no one specific supplement that I can pin point, it feels more of like an accumulative effort, but I'm definitely seeing improvement so I will continue with the current regiment. I do believe incorporating mushrooms into the mix will help (Chaga, reishi, lions mane, cordyceps). Like everyone here I have a whole pantry of failed supplements over the years. Nothing truly substitutes for a raw plant/fruit based diet, daily intensive exercise, and sunlight exposure, socializing with others. Those 4 things are the foundation.
On 30.01.2016 at 10:53 AM, Iamme. said:Has anyone made any solid progress going down the methylation pathway?
I've just contacted a practitioner who specialises in mineral analysis, have had a test done and it seems I am incredibly high in copper.
He has suggested detoxing this out through zinc and a few other supplements and at the same time working on methlaytion pathways using a supplement called TMG.
My guess is that for each of us who has suffered from accutane we have each had undermethylation as a genetic fault.
This prevented our livers from being able to detox the accutane properly. And previously why we had such bad skin as our livers could not detox anything properly hence the acne.
From there I believe the accutane stored in the liver caused a estrogen dominance which concurrently increased copper.
Copper is known to causes a whole bunch of symptoms, including what I awoke to this morning bleeding gums. This was a result of the antagonistic effect it has on vitamin c, resulting in some form of scurvy in my case. ( my diet as of late has been shocking and I have not had a nutritious meal in quite a few days, at least not what I should be having as I am constantly so depleted. )
- I have multiple symtpoms here that link up to copper toxicity and a general vitamin / mineral deficiency but what ever.This copper toxicity coupled with a still poor methlaytion cycle is what I beleive is causing all these problems in us.
I havent read this thread in a long time, only the last few pages but who has done what in terms of methylation and perhaps copper/hair mineral analysis?
Here are my results btw
.
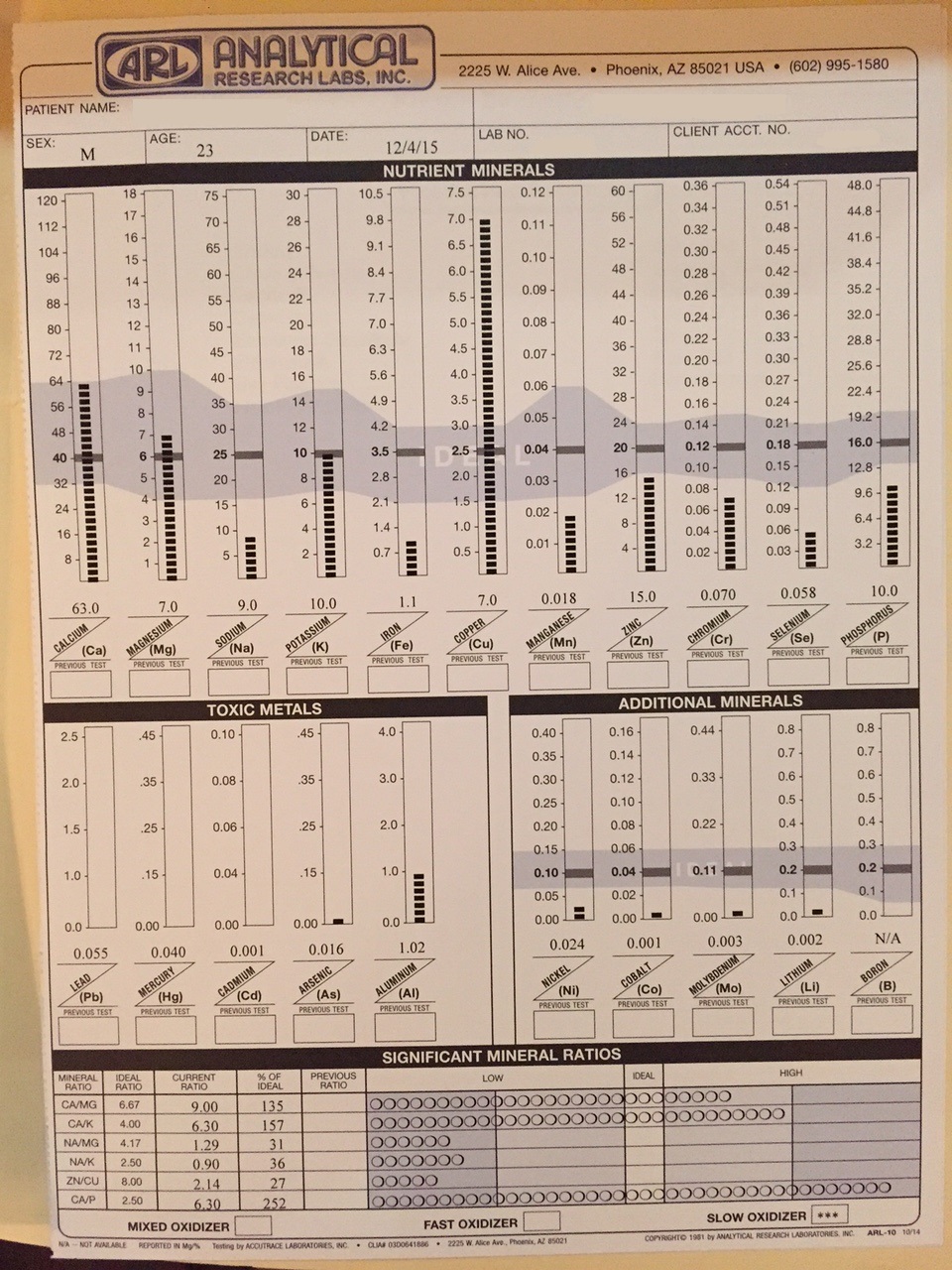
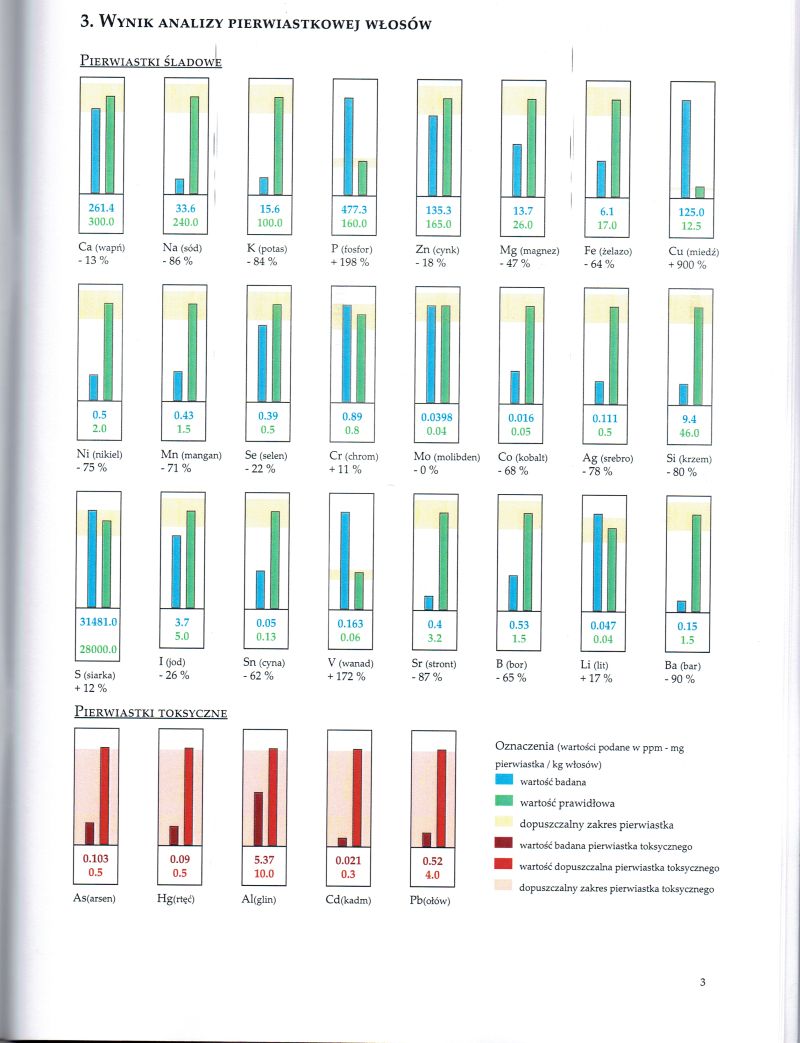
My hair analysis results are very similar to yours, especially the extremely high copper levels.
In one of your posts you said you pretty much fully recovered. What did you do to get better?
Also I see that you still have some gut issues and some pressure behind the eye. What helped me with that was getting a food allergy test and completely eliminating the bad ones out of my diet. A probiotic Lactobacillus Plantarum v299 was very beneficial too. The pressure is gone now and my gut is way better.
11 hours ago, macleod said:I did TRT last year from March to December. My blood tests showed low FSH and low T, which is a common pattern from what I've gathered from "taned brains" over the years. I'm fortunate enough to not have full on ED, but my libido was definitely a shadow of what it was pre tane. Yea, TRT is great...it makes your muscles feel tighter, your whole body tighter, leaner...erections upon waking up and a couple more throughout the day randomly. It's not bad being in the 1000 range when you've been at 200 for the past several years. I was so high towards the end of my cycle that the blood test couldn't even read the level, it just said >1000. It's pretty cool. But, it doesn't absolve clinical depression fully (at least for me). Although, cannabis has been helping lately, and I can tolerate more and more of it each day that goes by, which tells me I'm making improvements with my neurology.
When I asked my endo if there was a way to bring up FSH, he said no, there was not. however...
HMG is a fertility drug similar to HCG in use and some of its function, but also has the added benefit of FSH stimulation, while HCG is known mainly for LH stimulation. Your sex drive and sense of well being are restored as well as your potential for staying or becoming fertile (increased sperm count for men). The most significant difference between HCG and HMG is in the fact that HCG mimics LH (luetinized hormone). It gives the body a false signal that LH is present and everything else responds accordingly. HMG actually elevates natural LH. Now to some, theres little difference, but its always better when the body reacts in the most natural manner.
Well, regarding hormones, if that really is your priority, there is so much out there to try if you truly have a nothing to lose mentality. HCG, HMG, Test, HGH, Follistatin, Mifepristone, Clomid, oxytocin. And it is complicated. There's no right solution. The neuro endocrine system is super complex, so you either have to find an innovative knowledgeable physician that is willing to help (very difficult 1%) or you will have to trial and error on your own with the help of the internet (which isn't all bad if you find the right people/websites). I will try a couple of those on the list this spring/summer and try and give you my feedback, but I personally think my problems are more serotonin or dopamine related. But this summer should be fun. We will see.
This is interesting...my FSH has been at the bottom of the range since Ive been testing (2010). DHEA-S the same. Literally at the bottom of normal.
It appearsHMG is v. expensive (makes GH look cheap), which is why its not used really in TRT and HCG tends to restore fertility anyway.
I had an anti ageing Dr years ago, who diagnosed secondary hypogonadism, tried many protocols of a variety of hormones, with many losing effect after 2 weeks. I settled on low dose HCG weekly and pregnenolone for a couple of years, which got me to 4-5/10 from 1/10.
My current Dr withdrew everything recently though, as he feels my issues aren't hormonal and doesn't want to suppress anything. No pregnenolone even. He said this when I tested 500 T twice in a row (on no hormones). My most recent result (feeling no better) was 640, which was a shock, so perhaps he has a point. Sadly, this leaves little option in treating symptoms, unless I dr shop.
14 hours ago, Dubya_B said:Whole-genome sequencing is, or will soon be, cheap enough. The greater problem will be to find someone to officially analyze the data in the context of a scientific study; that is if there are enough volunteers getting tested among the post-Accutane community to generate a sufficient amount of data to be considered significant. And of course, there will be pompous dermatologists scoffing at the study anyway since it would be patient-generated data. Not as if their opinions would matter if we got a clean-cut set of genes that indicated an increased risk of side effects and possible therapeutic targets.Also, Accutane has little effect on circulating DHT levels, BUT a profound effect on peripheral 5ar activity. This is true of studies of skin biopsies taken after treatment and one study of type-1 5ar in the prostate during treatment.
There's reason to believe the negative effects of Accutane on 5ar-I observed in skin biopsies extend to the brain and central nervous system as seen in PFS. It's a shame that animal studies have not been performed on this point yet, but I would feel bad for any animal who was turned into a creature like me.
.... Noticed your DHEA-S was over the top high. That seems to be an almost across-the-board trait of post-Accutane people. Not sure why. ...Maybe persistently reduced negative feedback in HPA-axis as seen in the Accutane+Mifepristone study posted a few weeks ago?
Apologies in advance for this long post/reply.
Yes but it will be a start. Honestly the only reason I would want to know the genome sequencing is to determine whether PAS is associated with schizophrenia genes (I regard this as a worst case scenario). Given the connection between retinoids and schizophrenia, and the fact that many PAS symptoms are similar to the negative symptoms of schizophrenia. My hope here is the fact that PAS people don't have any of the positive symptoms of schizophrenia and that some people seem to experience sexual dysfunction without other typical symptoms, also I doubt many schizophrenics experience the sexual dysfunction that you get with PAS. If we can determine that, it would indicate that this is not caused by a direct problem/dysfunction of the dopaminergic system, but may be an issue with either the serotonergic system as in PSSD or in relation to 5AR inhibition as in PFS.
The only problem I find with the DHT/5AR hypothesis is that there seems to be far more PFS recoveries than PAS. Also treatment options which have shown some benefit for PFS people such as RU-486 seem to have little benefit sexually for the PAS people that have tried it (only 2 people so far, so maybe need bigger sample size). In fact I'm yet to see any truly, reliable PAS recoveries (So far I've noted 2 from the use of Finasteride, but they don't seem like full recoveries). When I use the term PAS here, I'm referring to the sexual side effects. But I agree that 5AR theory is a very plausible cause of PAS.
(Sorry im just going over this in my head) So what would you say? That in susceptible people 5AR activity gets completely fried in regions of the brain by accutane as happens in the skin. Leading to deficient 5AR activity in important regions of the brain associated with sexual drive etc.
Something that has always confused me is my resistance to the mental effects of steroids, like I want to know how the signal of serum testosterone is converted to dopaminergic signalling in the brain to produce a libido. Does the testosterone just directly stimulate androgen receptors on the dopamine neurons or is it first converted to DHT by 5AR and then stimulates dopamine activity. If the problem is 5AR, this would indicate that testosterone is a fairly weak stimulator of the androgen receptor alone as when its levels are raised by steroid use and not converted to DHT (provided the 5AR theory is correct) it is unable to elicit a response even at high dosages.
Saying that though, you would assume injecting DHT directly would solve the problem as it bypasses the 5AR. But as you say, DHT levels in the serum are normal. So either 5AR activity in brain regions is discrete from the serum, thus serum androgen levels have little effect on androgen levels and activity in particular brain regions or the loss of 5AR activity represents a problem not with a lack of testosterone or DHT activity but with a lack of neurosteroid production without which PAS develops as is likely the case in PFS.
One other strong point that this relates to 5AR is that the only drug to have reported to improve symptoms is Finasteride which clearly interacts with 5AR.
One other factor, dopaminergic drugs don't seem to effect me as strongly or in the same way as other people (this could be placebo/anecdotal) but when I take drugs such as cocaine, I seem to lack the euphoria that I imagine most people feel. I also used to tolerate/enjoy smoking weed far more before accutane but that seems to have changed (again this could be placebo and be an account of my general mood now). Dopaminegic agonist don't seem to boost sex drive/libido in people with PAS which you would assume bypasses the androgen activity. But again maybe a dopamine agonist alone isn't sufficient to stimulate libido and you need those 5AR products to really work libido and dopamine function in certain regions of the brain.
Yes DHEA-S are very high, this result does seem to be present in some PAS people. I've looked into it a little. I also started puberty fairly early and I believe DHEA-S are indicative of excessive adrenal steroid production which can lead to precocious puberty. So may be inconsequential.
Also dubya are you still in contact with paulo from the allthingsmale forum, he seemed to have a good brain on him. I think we need as many minds as possible working together on this.
24 minutes ago, mikez said:This is interesting...my FSH has been at the bottom of the range since Ive been testing (2010). DHEA-S the same. Literally at the bottom of normal.
It appearsHMG is v. expensive (makes GH look cheap), which is why its not used really in TRT and HCG tends to restore fertility anyway.
I had an anti ageing Dr years ago, who diagnosed secondary hypogonadism, tried many protocols of a variety of hormones, with many losing effect after 2 weeks. I settled on low dose HCG weekly and pregnenolone for a couple of years, which got me to 4-5/10 from 1/10.
My current Dr withdrew everything recently though, as he feels my issues aren't hormonal and doesn't want to suppress anything. No pregnenolone even. He said this when I tested 500 T twice in a row (on no hormones). My most recent result (feeling no better) was 640, which was a shock, so perhaps he has a point. Sadly, this leaves little option in treating symptoms, unless I dr shop.
If you have accutane induced sexual side effects such as low libido/interest in sex. Did the pregnenolone and HCG help with these sexual side effects at all?
Hello people,
I think its crazy that post Accutane people don't have a dedicated forum for Post Accutane Syndrome (PAS). All of the information is scattered throughout the internet on different forums rather than in one place. Additionally, though forums like this are great and worthwhile. The layout and lack of organisation makes content hard to find/read and makes real in depth discussion on specific topics difficult, as the thread is constantly interrupted by contrasting/unrelated/irrelevant posts.
The only chance that anything will be achieved in this dire situation is that we get better organised as a community. This will help to gain greater insights from blood results/experiments/experiences as well as increase the possibility of funding a future study or even recruiting study volunteers.
This is a work in progress, so there may be errors along the way but here is an attempt to make a forum dedicated to PAS - [removed]
I have also dedicated an area to the theories of PAS which I have tried to summarise, which may be of interest.
Also I don't post this to take anything away from this forum, we should continue to post here.
So do people that take excess copper or zinc have post copper/zinc syndrome?
or one of the founders of propecia help that had serious problems after taking milk thistle does he have post milk thistle syndrome?
Who's the guy on hack stasis again recommending copper and/or zinc?
Ive already spotted some people having some problems on there, looking through it briefly.
What Accutane did might not be specific to the drug itself.
Cations inhibit specifically type I 5 alpha-reductase found in human skin.
Abstract
Steroid 5 alpha-reductase catalyzes the reduction of testosterone into the very potent androgen dihydrotestosterone. Previously, we showed that human type I 5 alpha-reductase is expressed mainly in the skin, whereas a type II 5 alpha-reductase is more specifically expressed in the prostate. To assess the possible differential effects of various cations on the two types of 5 alpha-reductase, we constructed expression vectors and transfected them into SW-13 cells, a human adrenal carcinoma cell line containing negligible endogenous 5 alpha-reductase activity. The expressed 5 alpha-reductases were analyzed for their sensitivity to Li, Ca, Cd, Cu, Mg, Mn, Ni, Zn, and Fe. The results showed that type I 5 alpha-reductase was strongly inhibited by Cd, Cu, and Zn and moderately inhibited by Ni and Fe, with 50% inhibitory concentration values of 0.9, 1.9, 2.0, 169.2, and 174.3 microM, respectively. In contrast, type II 5 alpha-reductase activity was inhibited only by Cu, with a 50% inhibitory concentration value of 19.2 microM. The data showed that cations could specifically control 5 alpha-reductase activity expression, which is more strongly inhibited in a target tissue, especially the skin.
1 hour ago, guitarman01 said:So do people that take excess copper or zinc have post copper/zinc syndrome?
or one of the founders of propecia help that had serious problems after taking milk thistle does he have post milk thistle syndrome?
Who's the guy on hack stasis again recommending copper and/or zinc?
Ive already spotted some people having some problems on there, looking through it briefly.
What Accutane did might not be specific to the drug itself.Cations inhibit specifically type I 5 alpha-reductase found in human skin.
Abstract
Steroid 5 alpha-reductase catalyzes the reduction of testosterone into the very potent androgen dihydrotestosterone. Previously, we showed that human type I 5 alpha-reductase is expressed mainly in the skin, whereas a type II 5 alpha-reductase is more specifically expressed in the prostate. To assess the possible differential effects of various cations on the two types of 5 alpha-reductase, we constructed expression vectors and transfected them into SW-13 cells, a human adrenal carcinoma cell line containing negligible endogenous 5 alpha-reductase activity. The expressed 5 alpha-reductases were analyzed for their sensitivity to Li, Ca, Cd, Cu, Mg, Mn, Ni, Zn, and Fe. The results showed that type I 5 alpha-reductase was strongly inhibited by Cd, Cu, and Zn and moderately inhibited by Ni and Fe, with 50% inhibitory concentration values of 0.9, 1.9, 2.0, 169.2, and 174.3 microM, respectively. In contrast, type II 5 alpha-reductase activity was inhibited only by Cu, with a 50% inhibitory concentration value of 19.2 microM. The data showed that cations could specifically control 5 alpha-reductase activity expression, which is more strongly inhibited in a target tissue, especially the skin.
This is very interesting. I wonder is there are any minerals/supplements which significantly increase its activity?
23 hours ago, flynn said:If you have accutane induced sexual side effects such as low libido/interest in sex. Did the pregnenolone and HCG help with these sexual side effects at all?
Yes, low dose HCG (100IU) every 3 days and low dose pregnenolone (up to 20mg) daily. By 4-5/10 I meant in libido from 1/10.
On 3/9/2018 at 3:30 AM, Dubya_B said:Whole-genome sequencing is, or will soon be, cheap enough. The greater problem will be to find someone to officially analyze the data in the context of a scientific study; that is if there are enough volunteers getting tested among the post-Accutane community to generate a sufficient amount of data to be considered significant. And of course, there will be pompous dermatologists scoffing at the study anyway since it would be patient-generated data. Not as if their opinions would matter if we got a clean-cut set of genes that indicated an increased risk of side effects and possible therapeutic targets.Also, Accutane has little effect on circulating DHT levels, BUT a profound effect on peripheral 5ar activity. This is true of studies of skin biopsies taken after treatment and one study of type-1 5ar in the prostate during treatment.
There's reason to believe the negative effects of Accutane on 5ar-I observed in skin biopsies extend to the brain and central nervous system as seen in PFS. It's a shame that animal studies have not been performed on this point yet, but I would feel bad for any animal who was turned into a creature like me.
.... Noticed your DHEA-S was over the top high. That seems to be an almost across-the-board trait of post-Accutane people. Not sure why. ...Maybe persistently reduced negative feedback in HPA-axis as seen in the Accutane+Mifepristone study posted a few weeks ago?
Have you also confirmed the risk of sexual and reproductive side-effects are finally being printed on the PILS of all newly-manufactured boxes of Isotretinoin sold in Europe?
Seems pharmaceutical companies don't like to change the labels until they are coerced into doing it. Especially Roche.
One PIL I found. Note how they say you will recover and also how they say 'do nottake if you arehigh in Vit A - who the hell would know this?Theyshould be testing before treatment'.
https://www.medicines.org.uk/emc/product/3871/pil
One PIL I found. Note how they say you will recover and also how they say 'do nottake if you are high in Vit A - who the hell would know this?Theyshould be testing before treatment'.
On 3/9/2018 at 5:45 AM, TrueJustice said:Hows the Lions Mane going??I dont pretend to know as much as many of you here that post a lot of science and results etc but one area that we dont tend to dwell on enough is the nervous system and how it might be altered after tane. Sure weve discussed Vit B but what else can we look at??
I was listening to the radio today about people whove been bitten by venomous snakes who yes have lived to tell the tale ( no pun ) but are left with lingering nervous system issues years after, even little things like no sense of smell etc. My guess is you could substitute snake venom with Accutane - both are poisons yeah, both impact on the nervous system, Im suggesting we could have a problem with this system and we need to look into it more....
Macleod - you raised a similar point recently about the nervous system did you not, affected after tane?
Macleod - that is a good find - have you got a ref I coud look up?
yes to low T, low E, low FSH and LH